
004 - Working From Home?

The topics covered this week include:
🩺 Examination of a stoma
🩺 Acute pancreatitis
🌱 Tips for working from home
🔗 An interesting useful app!
Welcome to the fourth newsletter!
If you're a returning reader, welcome back! We’re now increasing in number!
If you’re new, welcome! You can have a look at the previous posts so you don’t miss anything!
The plan for this week's newsletter:
1- Surgical skill: Examination of a stoma
2- Surgical topic: acute pancreatitis
3- Productivity tip: working from home?
5- Interesting app: induction
Let's begin!
Surgical skill: Examination of a stoma
Stoma = Surgically created opening of a tube (bowel or urinary tract) to a body surface
A - Inspection
1- Check the site
Usually a colostomy is located in the left iliac fossa (LIF), whereas an ileostomy or urostomy is more likely to be found in the right iliac fossa (RIF).
2- Check the number of lumens
If it has 1 lumen and in RIF - then it is an end ileostomy or urostomy
If it has 1 lumen and in LIF - then it is end colostomy
If it has 2 lumens joined and in RIF - Loop ileostomy
If it has 2 lumens joined and in LIF - Loop colostomy
3- Also check for:
It if has a spout of it is flush to the skin
The effluent or bag contents
Surrounding skin quality
B - Palpation
Gently feel around the stoma site for any tenderness
Ask the patient to cough and feel for a cough impulse for any obvious parastomal hernia
Gently digitate the stoma to assess for any stenosis and check patency
C- Auscultation
Auscultate for bowel sounds
Absent bowel sounds might indicate ileus
High pitched tinkling indicates obstruction
D- Complete the examination
Ensure to cover the patient
Wash your hands
Thank the patient
Possible complications of stomas:
These can be classified as either specific or general
Specific complications
Ischemia
Parastomal hernia
Haemorrhage
Stenosis
Prolapse
General complications
Stoma diarrhoea - resulting in electrolyte imbalance (especially lowered potassium levels)
Malnutrition - vitamin B12 and iron deficiencies (absorbed at the terminal ileum and jejeunum respectively).
Renal complications plus gallstones - due to increased water loss and loss of bile salts (usually reabsorbed in terminal ileum)
Tip: keep practicing till you can do it absentmindedly.
It is quite important to practice surgical skills and examinations with someone till you reach a point where your examination and procedures flow smoothly. It will show that you’re confident and know what you’re doing.
Topic of the week: acute pancreatitis
Pancreatitis is inflammation of the gland parenchyma of the pancreas. For clinical purposes, it is useful to divide pancreatitis into acute, which presents as an emergency, and chronic, which is a prolonged and frequently lifelong disorder resulting from the development of fibrosis within the pancreas.
Definition: Acute pancreatitis is defined as an acute condition presenting with abdominal pain and is usually associated with raised pancreatic enzyme levels in the blood or urine as a result of pancreatic inflammation.
Incidence: It accounts for 3% of all cases of abdominal pain among patients admitted to hospital in the UK. The hospital admission rate is 9.8 per year per 100 000 population in the UK.
Worldwide, the annual incidence may range from 5 to 50 per 100 000.
The disease may occur at any age, with a peak in young men and older women.
Aetiology:
There is a really good mnemonic to remember the causes of acute pancreatitis. Once you memorise and revise this, you’re unlikely to forget it.
Mnemonic: I-GET-SMASHED
I - Idiopathic
G - Gallstones
E - Ethanol
T - Trauma
S - Steroids
M - Mumps, Malignancy (pancreatic cancer)
A - Autoimmune
S - Scorpion sting
H - Hypercalcemia, Hypertriglyceridemia
E - ERCP
D - Drugs
Clinical presentation:
Severe constant epigastric pain radiating to the centre of the back
Associated nausea and vomiting.
The patient may be distressed, sweating and mildly pyrexial.
Signs of guarding, tripod position seems of relieve pain.
Signs of shock is severe acute pancreatitis.
Uncommon: Bluish discolouration in the loins (Grey Turner’s sign) - only develops after several days
Blood investigations:
Serum amylase and lipase are diagnostic.
Serum lipase remains elevated for longer than serum amylase and is more specific, but less sensitive.
CRP (elevated)
FBC, LFT (show abnormality)
Radiological investigations:
Abdominal x-ray - can be performed but often show un-specific findings.
CT - may be required (shows pancreatic oedema, haemorrhage and necrosis).
Ultrasound scan - must be done within 48hours of admission to identify gallstone in the bile duct.
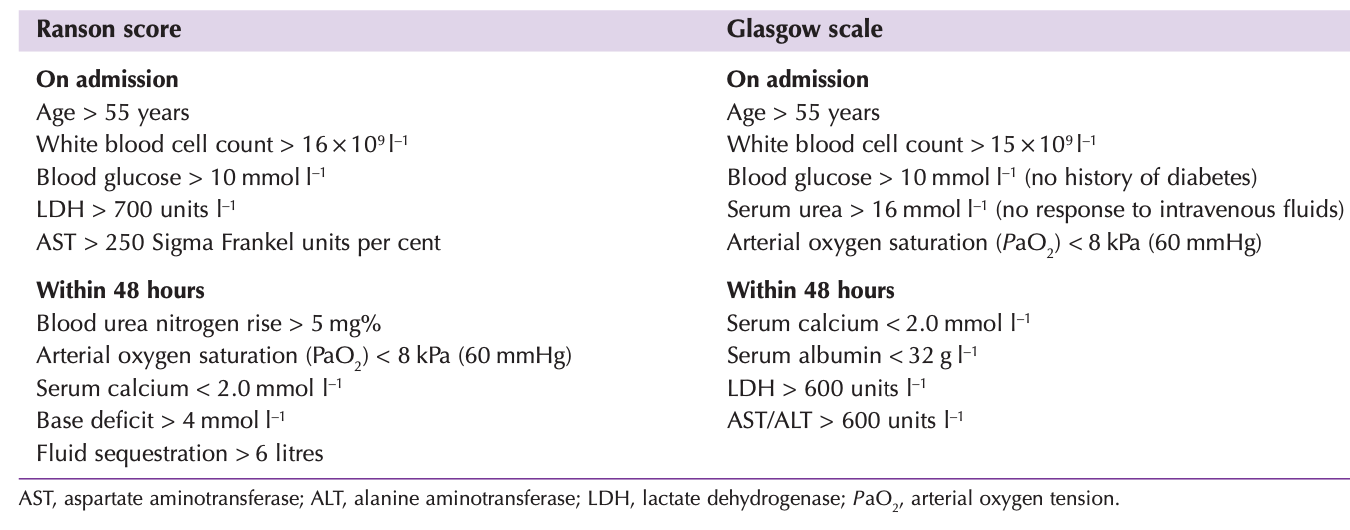
Assessing the severity of acute pancreatitis:
On account of the difference in outcome between patients with mild and severe disease, it is important to define that group of patients who will develop severe pancreatitis. Various scoring systems have been introduced, such as the Ranson and Glasgow scoring systems .
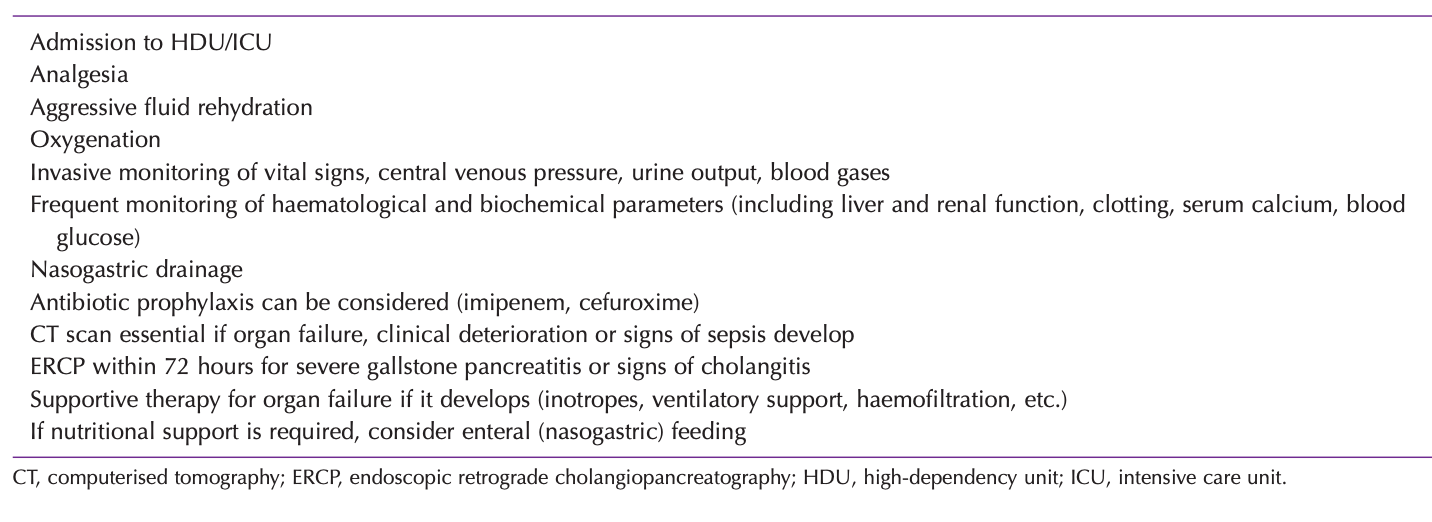
Early management of severe acute pancreatitis:
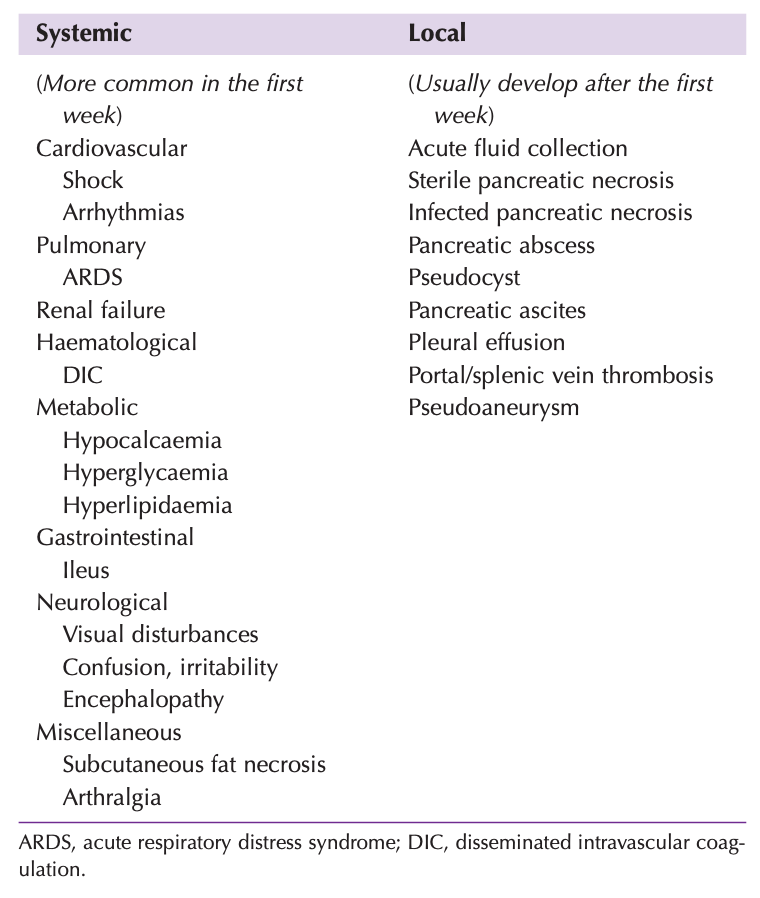
Complications of acute pancreatitis:
References:
1- Oxford Handbook of Clinical Surgery - 4th Edition
2- Basic surgical skills & techniques
3- Bailey and Love Short Practice of Surgery
Productivity tips - Working from home?
During the COVID-19 pandemic many of us have had to work from home. Balancing work with home lifestyle can be a challenge to many. It not only can be challenging to separate functional working hours, but you also don’t live alone at home and might even be sharing a room with siblings/roommates. Here are some tips that I have come across that might help:
1 - Spend a short amount of time writing out a list of all the goals you need to achieve and stick it somewhere visible near your working space (yes, please have a dedicated working space and avoid working near the TV or any other distractors).
2- When you wake up in the morning, make your bed. This is a tiny habit but it can help you achieve more during the day and you’re less likely to go back to sleep.
3- Have a nice cold/hot shower to wake yourself up in the morning.
4- Drink coffee/tea/whatever you like - don’t do this when already sitting to work. You deserve a few moments of peace and caffeine to start your day right. I usually drink some coffee first thing in the morning and take a cup of tea with me to the desk.
5- I read many articles and tips that keep saying to put your phone away and in the other room. Personally I don’t do this. I always have my phone with me at all times but consciously can avoid looking at it. It is all a matter of priorities. There is no point putting a phone away if you’re going to think about it. Check your messages, send whatever needs to be sent and just avoid your phone for an hour at least.
6- If you’re living with family/friends - then you can leave a sign at the door asking not to be disturbed/called for the duration of your work. Explain that you’re facing deadlines and should be left to work.
Interesting link/app
During on calls and daily rounds, we often find that we need to bleep other departments for consultations. I found out about an app that can be used in hospitals to get bleep numbers for the hospital you’re working in.
It is quite a productive way to save time connecting to other people within the NHS.
It is called induction.
This app can be downloaded as follows:
Do you have any specific surgical topic that you want to read about next week? You can always make suggestions as I plan to make this newsletter as useful to you as possible. Feel free to contact me at scrubsandsutures@gmail.com or on twitter and I will try to tailor the next one for you.
Thank you for reading and stay tuned for more topics next week!